Sigmund Freud was born on May 6, 1856 in Freiberg, Moravia which is now Czech Republic. Freud’s father was married three times and widowed twice. His father Jacob Freud, at the age of 39, married Sigmund’s mother, Amalia Nathanson, who was 19 years of age. Freud’s two step-brothers from his fathers first marriage was around the same age as his mother, therefore his oldest stepbrothers son was Freud’s first playmate as a child. Although there was seven younger children born, Sigmund remained his mother’s favorite. When Sigmund was four the family moved to Vienna. Freud’s early experiences in Vienna were very overwhelming due to the family being Jewish and the community being Catholic. He felt like an outsider. The standard for living was quite higher and educational opportunities were better in Vienna than the provinces. The area in which Sigmund’s family lived was called Leopoldstadt slum, which was rich in Jewish people. The housing there was cramped and they had to move quite often, once even with his fathers family. Freud went to a local elementary school and then attended the Sperl Gymnasium, a school that would prepare him for college from 1866 to 1873. Freud was a superior student and passed his final examination with flying colors, qualifying him for the University of Vienna at the age of seventeen. Even though housing was cramped, Sigmund’s parents recognized his scholarly achievement and Freud had his own room, while his siblings had to share a room. Sigmund lived with his parents until age 27, which was the custom at that time.
Freud received his doctor of medicine at the age of 24. He took seven years instead of the normal five acquiring his doctorate. Freud met Martha Bernays when he was 26 and were engaged two months later. They were separated during the most of the four years which preceded their marriage. Sigmund and Martha married in 1887. They had six children. One in particular, Anna, would become one of his most famous followers. Freud spent three years as a resident physician in the famous Allgemeine Krankenhaus, a general hospital and the medical center of Vienna. He spent five months in the psychiatry department. During the last part of Freud’s residency, he received money to pursue his neurological studies. Sigmund spent four months at the Salpêtrière clinic in Paris, France, under a neurologist named Jean Martin Charcot . This would interest Freud in hysteria.
Freud moved back to Vienna and started his own private practice in neurology. He devoted his efforts towards treating patients with hysteria by means of hypnosis. Joseph Breuer introduced Freud to a patient with hysteria, which became a well known case known as Anna O. Freud 39, introduced the term “psychoanalysis” and his work was well underway. At about this time Freud began a unique project, his own self-analysis, which he pursued primarily by analyzing his dreams. A major scientific result was The Interpretation of Dreams (1901). Freud had developed his therapeutic technique, dropping the use of hypnosis and shifting to the more effective and more widely applicable method of "free association." In 1923 Freud developed a cancerous growth in his mouth, which eventually led to his death sixteen years and thirty-three operations later. In spite of this, these were years of great scientific productivity. He published findings on the importance of aggressive as well as sexual drives ( Beyond the Pleasure Principle, 1920); developed a new theoretical framework in order to organize his new data concerning the structure of the mind ( The Ego and the Id, 1923); and revised his theory of anxiety to show it as the signal of danger coming from unconscious fantasies, rather than the result of repressed sexual feelings ( Inhibitions, Symptoms and Anxiety, 1926). Freud spent his last year in London, England, undergoing surgery. He died on September 23, 1939. The influence of his discoveries on the science and culture of the twentieth century is limitless.
Sigmund Freud, the father of psychoanalysis, was born on May 6, 1958 in Freiberg, Moravia. When he was four or five years old his family moved to Vienna, where he lived most of his life. Sigmund was a very smart child always at the head of his class. He attended medical school, where he began his research mainly focusing on neurophysiology.
Freud is said to have made the idea of the conscious vs. unconscious mind popular. The conscious mind is what a person is aware of at any time: your present perceptions, memories, thoughts, fantasies, and feelings. The largest part according to Sigmund is the unconscious. It includes all the things that are not easily available to awareness, including many things that have their origins there, such as our drives and instincts, and things that are put there because we don’t like to look at them, such as memories and emotions associated with trauma. Freud said that the unconscious is the source of our motivations, ranging from simple desires for food or sex, neurotic compulsions, or the motives of an artist.
According to Sigmund Freud's psychoanalytic theory of personality, personality is composed of three elements. These three elements of personality known as the id, the ego and the superego work together to create complex human behaviors. According to Freud, we are born with our Id. The id is a big part of our personality because as newborns, it allows us to meet our basic needs. Freud believed that the id is based on our pleasure principle. The id wants whatever feels good at the time, with no consideration for the reality of the situation. When a child is hungry, the id wants food, and therefore the child cries. When the child needs to be changed, the id cries. When the child is uncomfortable, in pain, too hot, too cold, or just wants attention, the id talks until his or her needs are met.
The id doesn't care about reality, about the needs of anyone else, only its own satisfaction. If you think about it, babies are not real considerate of their parents' wishes. They have no care for time, whether their parents are sleeping, relaxing, eating dinner, or bathing. When the id wants something, nothing else is important.
Within the next three years, as the child interacts more with the world, the second part of the personality begins to develop. Freud called this part the Ego. The ego understands that other people have needs and desires and that sometimes being impulsive or selfish can hurt us in the long run. It’s the ego's job to meet the needs of the id, while taking into consideration the reality of the situation.
By the age of five the Superego develops. The Superego is the moral part of us and develops due to the moral and ethical restraints placed on us by our caregivers. Many associate the superego with the conscience as it dictates our belief of right and wrong.
In a healthy person, according to Freud, the ego is the strongest so that it can satisfy the needs of the id, not upset the superego, and still take into consideration the reality of every situation. If the id gets too strong, impulses and self-gratification take over the person's life. If the superego becomes too strong, the person would be driven by rigid morals, would be judgmental and unbending in his or her interactions with the world.
Jean Piaget was born on August 9, 1896, in Neuchatel, Switzerland. He is the oldest child of Arthur Piaget and Rebecca Jackson. Piaget was a Swiss biologist, philosopher, and psychologist best known for his work in the area of developmental psychology. He died on September 17, 1980, in Geneva Switzerland and is still buried there today.
At age ten he had already published his first paper, and by age 22 he had received his Ph.D. in science from the University of Neuchatel. In 1925, Piaget, took the chair of philosophy at the University of Neuchatel; his duties where to teach psychology, philosophy, science, a philosophy seminar, and sociology. Also at this time, his first daughter was born. His second daughter was born in 1927 and a boy followed in 1931. With the birth of his children he started to spend considerable time, with the help of his wife, observing their reactions and subjecting them to various experiments. He looked at the genesis of intelligent conduct, ideas of objective constancy, and causality. He also noted symbolic behaviors such as imitation and play. The main benefit that he derived from these studies was that Piaget learned in the most direct way how intellectual operations are prepared by sensory-motor action, long before the appearance of language. With this knowledge he changed his method of study by modifying the direction of conversation to objects that the child could manipulate by themselves. He discovered that children up to the age of twelve did not believe in the constancy of material quantity, weight, and volume of a lump of modeling clay. He had also discovered from his own children that between the ages of six to ten months, they did not possess the notion of constancy and permanency of an object disappearing from view. He felt that there had to be successive stages in the development of ideas of constancy which could be studied in concrete situations rather than solely through language.
Piaget was originally trained in the areas of biology and philosophy. He considered himself a "genetic epistemologist" with his main interest being how one comes to know things. Piaget felt that the difference between humans and animals was the fact that humans are able to do reasoning through abstract symbolism. Piaget was interested in the thought processes that underlie reasoning and felt that younger children answered differently than their older peers due to the fact that the reasoned differently. From this, he observed children of various ages and development the Process of Cognitive Development which has two major aspects: the coming to know and the stages that we move through to acquire this ability.
The four stages of Piaget’s Cognitive Development consist of: the sensorimotor stage, the preoperational stage, the concrete operational stage, and the formal operational stage. The sensorimotor stage ranges from birth to nearly two years in which you experience the world through senses and actions (looking, hearing, touching, mouthing, and grasping). The preoperational stage ranges from age two to about six or seven years; this is when you represent things with words and images using intuitive rather than logical reasoning. The concrete operational stage ranges from age seven to eleven years and is when you start to think logically about concrete events; grasping concrete analogies and performing arithmetical operations. Finally, the formal operational stage ranges from twelve years through adulthood and is when you begin to reason abstractly.
Burrhus Fredric Skinner or more commonly called B.F. Skinner was one of the most influential American psychologists of all time. He was born on March 20th 1904 in a small town called Susquehanna located in Pennsylvania. His father was a lawyer and his mother was a housewife. He spent much of his childhood building things. For example he and a friend built a cabin in the woods.
After High School he decided to attend Hamilton College. He did not fit in very well there; he did not enjoy the fraternity parties or the football games. B.F. wrote for school paper, including articles critical of the school and the faculty. Upon graduation Skinner decided to become a writer. Moving back home he did not write much. His entire production from the period he called his "dark year." This year consisted of a dozen short newspaper articles and a few models of sailing ships. After this “dark year” Skinner decided to go to New York City for a few months. Working as a bookstore clerk, he started reading books by Pavlov and Watson. He was very impressed and excited about what they did and wanted to learn more.
So, at the age of 24 Skinner enrolled in the Psychology Department of Harvard University. Still rebellious and impatient with what some considered unintelligent ideas, Skinner found a person that was willing to mentor him. His name was William Crozier; he was the chair of a new department of Physiology.
During his time at Harvard he built new equipment and started doing one of his most famous experiments with rats. Skinner constructed apparatus after apparatus as his rats' behavior suggested changes. After a few changes to the apparatus and some lucky accidents Skinner invented the cumulative recorder. This is a mechanical device that recorded every response as an upward movement of a horizontally moving line. The slope showed rate of responding. Skinner discovered that the rate with which the rat pressed the bar depended not on any preceding stimulus (as Watson and Pavlov had insisted), but on what followed the bar presses. This was a new discovery. Unlike the reflexes that Pavlov had studied, this kind of behavior operated on the environment and was controlled by its effects. Skinner named it operant behavior.
In 1936, then 32 years old, Skinner married Yvonne Blue and the couple moved to Minnesota where Skinner had his first teaching job. In 1944 World War II was in full swing. Airplanes and bombs were common, but there were no missile guidance systems. Skinner was willing to do what he could to help and sought funding for a top secret project to train pigeons to guide bombs. He trained pigeons to keep pecking a target that would hold a missile onto a target. The Project Pigeon was discontinued but, the work was useful.
In 1945, Skinner and his family moved to Bloomington Indiana where he became Chair of the Psychology Department at Indiana University. Then in 1989 he was diagnosed with leukemia, but kept as active as he could. At the American Psychological Association, about 10 days before he died, he gave a talk before a crowded auditorium. He passed away August 18th 1990.
Have you ever been around someone with Alzheimer’s? If not you don’t really realize how bad of disease it is. I have always know what it was and that the person for got everything, but didn’t know much about it until my grandma got it. The only good thing about Alzheimer’s is that it is a painless death. Unlike most diseases Alzheimer’s is incurable. They have pills to help with it and slow the process down but never get rid of it.
Alzheimer’s has seven stages. The first four stages aren’t very sever and you wouldn’t think much about it being Alzheimer’s as to getting old, or just forgetting something. The first stage really isn’t even a stage it’s just normal behavior. The second stage is when the person feels like they are forgetting things but no one notices it but themselves. In the third stage is when family members start noticing Alzheimer’s. Now that Alzheimer’s has started showing symptoms you can start to tell the decline in memory. In the fourth stage they start forgetting recent events and how to do simple tasks. Then stage five comes and they can’t recall where they went to school, what there address is, or what day it is. Stage six is the second to last stage. In this stage they forget their history, and their family members. They also will need help getting dressed and using the toilet, and may wonder around. The last and final stage is stage seven. In the last stage they need help with everything and are unable to have a conversation.
Alzheimer’s is an incurable disease but there are some things you can do to slow the process down. Doctors can give u a pill that slows the process but some people get nightmares and cannot take the pill. For those people there is an off breed pill that isn’t as strong but they won’t get nightmares and still helps with the disease. Some other things that you can do to help are not to criticize them. For example don’t argue by telling them you told them and they just don’t remember. Don’t remind them they forgot, or question something you had just told them. Things you should do to help are repeating instructions and give them time to comprehend it. You should accept the blame when something is wrong even if you have no clue what their talking about. Also it is good to keep them physically active and doing things. Once they quit doing things the process speeds up.
Alzheimer’s is a very serious disease even though it doesn’t seem like it since all that happens is them forgetting. It affects everyone else’s lives around them. It is harder on my grandpa than my grandma who has Alzheimer’s, because she asks him the same questions fifty times a day and it gets really annoying having to repeat yourself. There are many ways to help with Alzheimer’s since you can’t cure it. I hope you have learned how serious this disease is.
Music and the Mind
Bob Schroeder
Music has been and is a large part of society. Dating back to the birth of music, back nearly as far as the beginning of human beings, we see that it has always been a major part of Earth’s cultures around the world. But why are we drawn so easily to music; moreover, why are certain people drawn to certain types of music? Recent studies have uncovered many new findings about how music can influence our minds, bodies, and even our very lives. To put this in perspective, music defines who we are and what we stand for.
Norman M. Weinberger, Ph.D., professor of neurobiology and behavior at the University of California at Irvine, claims that, “music seems to be a part of our biological heritage.” For example, infants “listen” and even understand music as their mother sings to them. According to Weinberger, our brains have evolved to adapt to music, but not in one specific way. He even states, “Because music has many elements—rhythm, melody and so on…. certain cells in the right hemisphere respond more to melody than to language.” Furthermore, neurons can learn to recognize some sounds which can stimulate a person’s emotions and mood.
Musical experience can be beneficial to one’s learning ability, motor skills, health, overall intelligence, etc. Doctor Weinberger states that musical experience can also “shape” the brain in a way. In his example he makes the claim that, “the cortical representation of digits 2 to 5 on the left hand of string players is greater than for the right, suggesting that musical experience does influence the brain. Similarly, findings indicate that merely listening to music can influence the brain. Research done by Shaw and colleagues reported on the Mozart Effect “… finding that college students who listen to Mozart for 10 minutes perform better on spatial-temporal tests, like pattern matching.” Yet, they also go on to say that the effects are minimal and short lived.
But don’t forget that music has long term effects as well with “time and practice.” According to an article from PsychologyToday.com, "Evidence suggests that long-term musical involvement reaps cognitive rewards in language skills, reasoning and creativity and boosts social adjustment. Music exercises the brain. Playing an instrument, for instance, involves vision, hearing, touch, motor planning, emotion, symbol interpretation…all of which activate different brain systems. This may be why some Alzheimer's patients can perform music long after they have forgotten other things."
In the following video, it is explained where and how music affects the brain.
Because of music’s role in the brain, some believe that it can be a form of medicine. The American Music Therapy Association is an organization designed to provide/promote therapy with music. For instance, music therapy interventions can be designed to:
In the following video Author and Neurologist Oliver Sacks experiments on how music “lights” up the brain. In the video, it is shown that, when a desired music is listened to, the brain lights up in many areas including the amygdala (processes emotions). It is truly astounding how much music can influence our bodies, minds, and life! There are so many unopened doors within the psychology of music. Maybe one day, we will find that music is much more powerful than we now perceive it to be.
Sleep Disorders
Most people go through times when it’s hard to fall asleep or wake up in the middle of the night. College students are the most sleep deprived individuals so it’s normal to feel fatigued in midday. Although when sleep loss continues on for months and inhibits your daily living abilities, you may be dealing with a sleep disorder. If you’re having trouble sleeping, you’re not alone. According to the National Commission on Sleep Disorders Research, at least 40 million Americans suffer from chronic, long-term sleep disorders and another 20 to 30 million experience occasional sleep problems. A lack of quality sleep can have a negative impact on your energy, emotional balance, productivity, and health.
Insomnia, the inability to get to sleep or sleep well at night, is an all-too common sleeping problem. Insomnia can be caused by a variety of things including stress, jet lag, a health condition, the medications you take, or how much caffeine you consume over the day. Insomnia can also be caused by other sleep disorders or mental health conditions such as anxiety and depression. One of the common remedies for this is sleeping pills or alcohol, but this can be harmful as they reduce REM sleep.
Narcolepsy is a sleep disorder that involves excessive, uncontrollable daytime sleepiness. It is caused by a dysfunction of the brain mechanism that controls sleeping and waking. Narcoleptics may have “sleep attacks”, which usually last less than 5 minutes, while in the middle of talking, working, or even driving.
Sleepwalking has been described in medical literature dating before Hippocrates (460 BC-370 BC). In Shakespeare's tragic play, Macbeth, Lady Macbeth's famous sleepwalking scene is ascribed to her guilt and resulting insanity as a consequence of her involvement in the murder of her father-in-law. Sleepwalking characteristically occurs during the first or second sleep cycle during stages 3 and 4 and is characterized by walking while asleep. Occasionally nonsensical talking may occur while sleepwalking. The person's eyes are commonly open but have a glassy "look right through you" character. This activity most commonly occurs during middle childhood and young adolescence. Approximately 15% of children between 4-12 years of age will experience sleepwalking. Generally sleepwalking behaviors are resolved by late adolescence, although approximately 10% of all sleepwalkers begin their behavior as teens. Studies have indicated there is a genetic connection.
Sleep apnea is another sleeping disorder that occurs in 1 out of 20 people. Apnea, or no breath, Is when people stop breathing during their sleep. After a minute or so they’re blood oxygen level drops and they wake up. While most people with sleep apnea don’t remember these awakenings, but feel the effects in other ways, such as exhaustion during the day, irritability and depression, and decreased productivity. Sleep apnea is a serious, and potentially life-threatening, sleep disorder. Sleep apnea can be successfully treated with Continuous Positive Airway Pressure (CPAP), a mask-like device that delivers a stream of air while you sleep. Losing weight, elevating the head of the bed, and sleeping on your side can also help in cases of mild to moderate sleep apnea.
Imagine waking up and not being able to move. As you lie there you can feel someone or something evil in the room with you. Without being able to even call out for help you feel like your being crushed. After a few long seconds of complete terror you can move again , everything is normal and your room is empty. This is a example of what is like to experience sleep paralysis.
Sleep paralysis is a sleep disorder that occurs entering or coming out of REM sleep. REM sleep is part of the sleep cycle which stands for Rapid Eye Movement. During sleep the brain makes the muscles relax and keeps them from moving, this is called atonia. REM sleep is also the closest to conciseness of the sleep cycle. In some cases a person can wake up without the brain sending the signal to the body move again which is sleep paralysis. People experiencing sleep paralysis is not able to move any part of their body or talk. They are able to look around a little bit and breath. During the episode people say that it feels like something heavy is holding them down. People also become extremely anxious to the point of terror. Most people say that they feel a presence in the room that they can’t look to see almost always described as malevolent or evil. Some experience hallucinations, seeing grey or dark figures in the room or sitting on their chest trying to crush them. The episodes last anywhere from a few seconds to a few minutes. The episodes can normally be stopped sooner by being touched or extreme effort to move.
Most people that experience sleep paralysis also have narcolepsy, but anyone can experience it and most will at least once. There are a few things that help lead to sleep paralysis. Lack of sleep or not having a consistent sleep schedule. It is more frequent when people are sleeping on their back. Sleep paralysis is not extremely dangers and most people can live with having multiple experiences a month.
works cited: www.sleepeducation.com/Disorder www.sleepdeeper.net
Autistic Spectrum Disorders
by Kristin Mann
Autism, a complex brain disorder that constrains a person’s ability to communicate and develop social relationships, is one of three types of Autism Spectrum Disorder (ASD). Spectrum disorders affect people in different ways and can range from very mild to severe. “Classic” autism is what most people think of when they hear the word autism. The other two types of ASDs are Asperger Syndrome; which is a milder version of autism; and Pervasive Developmental Disorder-Not Otherwise Specified (PDD-NOS); which is the mildest version of autism in which case the individual meets some, but not all, of the criteria for autism. ASDs present before three (3) years of age and continue throughout the lifetime. Some children with Autism show signs within a few months of birth; others don’t start showing signs until 24 moths or after. A child with ASD can develop normally until around 18-24 months of age, at which point they will stop gaining new skills or lose the ones they already mastered.
Early detection signs of ASDs include:
No response to their name by 12 months
Don’t point to objects they want or are interested in by 14 months
The absence of pretend play by 18 months
Avoidance of eye contact and desire to be alone
Inability to understand others feeling or state their own
Delayed Speech and language skills
Echolalia-the repeating of words or phrases
Communicate unrelated answers when asked questions
Minor changes cause discomfort
Obsessive interests or interactions
Stimming- flapping of hands, rocking of the body, toe walking, spinning in circles for a length of time, stacking or lining up of objects, etc.
Unusual reactions when their 5 senses are involved (touch, smell, taste, sound,see)
ASDs are difficult to diagnose because there are no definitive medical tests that affirm the disorder. One’s behavior and development are the only diagnostic tools doctors can use when pronouncing an ASD diagnosis. There is NO cure foe Autism. Research indicates that early treatment services; such as speech therapy, can greatly improve an autistic child’s development. The Diagnostic and Statistical Manual of Mental Disorders (DSM IV) breaks down autism disorder into three levels. Level 1, the most severe, has to have at least 6 items listed in three sub categories; at least two from category A, and at least one each from categories B and C. Category A consists of qualitative impairments in social interaction, category B consists of qualitative impairments in communication, and category C consists of restrictive, repetitive, and stereotyped patterns of behavior, interests and activities. A level 2 envelopes delays or abnormal functioning in at least one of the following areas with onset prior to three years of age; Social interaction, language as used in social communication, and symbolic or imaginative play. The third level, and least severe illustrated a disturbance that in not better account for my Rett’s Disorder (a neurodevelopmental disorder that affect females almost exclusively) or Childhood Disintegrative Disorder (a disorder similar to Autism ).
Many different influences can contribute to an ASD diagnosis ranging from environmental, biological, and genetic factors. As of yet the precise causes of ASDs are unknown. Scientists agree that genetics play a big role in the likelihood of an ASD diagnosis. Children with ancestral ASD diagnosis’ are at a higher risk of having an ASD. Approximately 10% of ASD patients also have other identifiable genetic disorders consistent with Fragile X syndrome, tuberous sclerosis, Trisomy 21 and other chromosomal abnormality disorders. Some teratogens ingested during pregnancy have also been linked with higher risks of ASD, for example the prescription drug Thalidomide (a sedative used in the 1950’s) and Valporic Acid (an anticonvulsive or mood-stabilizing drug). It is now known that nurture has nothing to do with an ASD diagnosis. However, concerns about certain vaccines and infections have led researchers to consider these as risk factors.
Work Cited:
Division of Birth Defects, National Center on Birth Defects and Developmental Disabillities, Centers for Disease Control and Prevention. "CDC - Facts, Autism Spectrum Disorders - NCBDDD." Centers for Disease Control and Prevention. 29 Dec. 2010. Web. 20 Apr. 2011. <http://www.cdc.gov/ncbddd/autism/facts.html>.
"Autism Speaks, Press Updates, Autism Speaks and the World's Leading Autism Experts Announce the Publication of the Autism Genome Project Phase 1 Results." Autism Speaks, Home Page. Web. 20 Apr. 2011. <http://www.autismspeaks.org/press/agp_results.php>.
Spina Bifida
Katie Clancy and Caity Patterson
Spina bifida is a birth defect that involves the incomplete development of the spinal cord or its coverings. The term spina bifida comes from Latin and literally means "split" or "open" spine.
Spina bifida occurs at the end of the first month of pregnancy when the two sides of the embryo's spine fail to join together, leaving an open area. In some cases, the spinal cord or other membranes may push through this opening in the back. The condition usually is detected before a baby is born and treated right away.
The causes of spina bifida are largely unknown. Some evidence suggests that genes may play a role, but in most cases there is no family connection. A high fever during pregnancy may increase a woman's chances of having a baby with spina bifida. Women with epilepsy who have taken the drug valproic acid to control seizures may have an increased risk of having a baby with spina bifida.
The two forms of spina bifida are spina bifida occulta and spina bifida manifesta. Spina Bifida Occulta is the mildest form of spina bifida (occulta means hidden). Most children with this type of defect never have any health problems, and the spinal cord is often unaffected. Spina Bifida manifesta includes two types of spina bifida: Meningocele involves the meninges, the membranes responsible for covering and protecting the brain and spinal cord. If the meninges push through the hole in the vertebrae (the small, ring-like bones that make up the spinal column), the sac is called a meningocele. Myelomeningocele is the most severe form of spina bifida. It occurs when the meninges push through the hole in the back, and the spinal cord also pushes though. Most babies who are born with this type of spina bifida also have hydrocephalus, an accumulation of fluid in and around the brain.
Because of the abnormal development of and damage to the spinal cord, a child with myelomeningocele typically has some paralysis. The degree of paralysis largely depends on where the opening occurs in the spine. The higher the opening is on the back, the more severe the paralysis tends to be. Children with spina bifida often have problems with bowel and bladder control, and some may have attention deficit hyperactivity disorder (ADHD) or other learning difficulties, such as hand-eye coordination problems. Doctors also may use ultrasound to see if a baby has spina bifida; in some cases, the spinal defect can be seen on the ultrasound study. Amniocentesis also can help determine whether a baby has spina bifida. A needle is inserted through the mother's belly and into the uterus to collect fluid that is tested for AFP.
Maternal folic acid deficiency has been linked to spina bifida, and researchers believe that many cases can be prevented if women of childbearing age consume 0.4 milligrams (400 micrograms) of folic acid every day, and continue to take it throughout the first trimester.
It is important that folic acid consumption start before the onset of pregnancy to provide the best protection. Good sources of folic acid include eggs, orange juice, and dark green leafy vegetables. Many multivitamins contain the recommended dose of folic acid, too.
Babies who are born with spina bifida occulta often have no outward signs or symptoms. The spinal cord does not protrude through the skin, although a patch of hair, a birthmark, or a dimple may be present on the skin over the lower spine. Children with spina bifida occulta seldom need treatment.
But other forms of the disease have obvious signs. Babies who are born with the meningocele form have a fluid-filled sac visible on the back. The sac is often covered by a thin layer of skin and can be as small as a grape or as large as a grapefruit.
Babies with myelomeningocele also have a sac-like mass that bulges from the back, but a layer of skin may not always cover it. In some cases, the nerves of the spinal cord may be exposed. A baby who also has hydrocephalus will have an enlarged head, the result of excess fluid and pressure inside the skull.
In cases of spina bifida manifesta, treatment depends on the type of spina bifida and its severity. Babies with meningocele usually have an operation during infancy in which doctors push the meninges back and close the hole in the vertebrae. Many will have no other health problems later unless there is nerve tissue involved with the sac. Babies with myelomeningocele need more immediate attention and often have surgery within the first 1 to 2 days after birth. During this first surgery, doctors push the spine back into the vertebrae and close the hole to prevent infection and protect the spine.
A baby who also has hydrocephalus will need an operation to place a shunt in the brain. The shunt is a thin tube that helps to relieve pressure on the brain by draining and diverting extra fluid. In addition, some children need subsequent surgeries to manage problems with their feet, hips, or spine.
The location of the gap in the back often dictates what kind of adaptive aids or equipment a child with myelomeningocele will need. Those with a gap high on the spinal column and more extensive paralysis often need to use a wheelchair, while those with a gap lower on the back may be able to use crutches, leg braces, or walkers.
Parents of children with spina bifida receive support from a medical team that may include several doctors (such as neurosurgeons, urologists, orthopedic surgeons, rehabilitation specialists, and general pediatricians), a nurse practitioner, physical and occupational therapists, and a social worker.
The goal is to create a lifestyle for the child and family in which the disability interferes as little as possible with normal everyday activities.
Andrea is 12 years old and in the 6th grade. She likes to go swimming, play with her dog, and have friends over. She's been in three dance recitals, and she even received a standing ovation once. She's traveled to Canada and many places in the United States, and next summer she hopes to go to Scotland. When she's older, Andrea wants to be a chef. Like you, Andrea is interested in many things and can do a lot of stuff. What might be different from you, though, is the fact that Andrea can't walk. Andrea has spina bifida (say: spy-nuh bih-fuh-duh) and uses a wheelchair to get around.
There is no cure for SB because the nerve tissue cannot be replaced or repaired. Treatment for the variety of effects of SB may include surgery, medication, and physiotherapy. Many individuals with SB will need assistive devices such as braces, crutches, or wheelchairs. Ongoing therapy, medical care, and/or surgical treatments may be necessary to prevent and manage complications throughout the individual's life. Surgery to close the newborn's spinal opening is generally performed within 24 hours after birth to minimize the risk of infection and to preserve existing function in the spinal cord.
The prognosis for individuals with SB depends on the number and severity of abnormalities. Prognosis is poorest for those with complete paralysis, hydrocephalus, and other congenital defects. With proper care, most children with SB live well into adulthood.
The NINDS supports a broad range of research on neural tube defects such as SB aimed at finding ways to treat, prevent, and, ultimately, cure these disorders. Recent studies have shown that the addition of folic acid to the diet of women of child-bearing age may significantly reduce the incidence of neural tube defects. Therefore it is recommended that all women of child-bearing age consume 0.4 mg of folic acid daily.
Post-traumatic stress disorder, or PTSD, Is an anxiety disorder that usually occurs after you experience a traumatic event such as war, natural disaster, or even a prison stay. As of 2005 more than 200,000 veterans suffered from this disorder. The duration of the event or number of traumatic events someone goes through can put a person at more of a risk developing this problem. The disorder usually gets better after the traumatic event happens after three months but for some people it can last for years. PTSD can affect anyone at any age that has a life changing event happen. It can drive people that it affects to turn to alcohol and drug abuse.
What causes this disorder is still not really known but it changes how the responds to stressful things. Using a support group can help protect from dealing with PTSD. People who live with PTSD relive the bad event that happened to them. They will have bad dreams of it, flashbacks, or get up set on the anniversary of the event.
PTSD has many symptoms that can go with it and are divided into three different categories.
Reliving the event
• Flashbacks, they think the event is happening again
• Have reoccurring dreams of it
• Reactions to events or situations that remind them of the event
Avoidance
• Feel like you don’t care about anything
• Detachment
• No interest in normal activities
• Less expression in there moods
• Have the feeling of having no future
Arousal
• Have difficulty concentrating
• Exaggerated response to startling things
• Heightened awareness
• Problems sleeping
PTSD can be treated and reduce the symptoms that the person may experience. Trying to talk about the event to a friend or a family member can help someone to live with this or another PTSD survivor. They try to make the patient recall the event that happened to them and get them to express their feelings to get control over the experience. This helps the person to get of the mourning stage of the event. If the person is battling depression, alcoholism, or drug abuse though, they have to get these problems treated before they can tackle their PTSD problem.
Obsessive-Compulsive Disorder and What It Is
By Rusty Bohrer
Obsessive-Compulsive Disorder is an anxiety disorder in which you have unreasonable thoughts and fears and the need to do a ritual or a organized plan. People with this disorder suffer from experiencing repeated obsessions that interfere with a person's ability to function in a social, occupational, and educational settings. Obsessive-compulsive disorder often centers around thoughts, such as a fear of getting covered in germs. To ease your contamination fears, you may compulsively wash your hands until they're sore and chapped. Despite the efforts of many people, thoughts of obsessive-compulsive behavior keep coming back. This may lead to more ritualistic behavior, and a savage cycle that's typical of obsessive-compulsive disorder.
There are four types of obsessions that are aggressive, sexual, religious or harm related with checking compulsions, obsessions that are about balance accompanied by arranging or repeating compulsions, and symptoms of hoarding.
Obsessions often have themes to them, such as:
Having things orderly and symmetrical
Aggressive or horrific impulses
Sexual images or thoughts
OCD symptoms involving obsessions may include:
Fear of being contaminated
Doubts that you've locked the door or turned off the stove
Thoughts that you've hurt someone in a traffic accident
Intense distress when objects aren't orderly or facing the right way
Images of hurting your child
Impulses to shout obscenities in inappropriate situations
Avoidance of situations that can trigger obsessions such as shaking hands
Dermatitis because of frequent hand washing
Skin lesions because of picking at your skin
Hair loss or bald spots because of hair pulling
As with OCD obsessions, compulsions typically have themes, such as:
Washing and cleaning
Counting
Checking
Demanding reassurances
Performing the same action repeatedly
Orderliness
OCD symptoms involving compulsions may include:
Hand washing until your skin becomes raw
Checking doors repeatedly to make sure they're locked
Checking the stove repeatedly to make sure it's off
Counting in certain patterns
Making sure all your canned goods face the same way
The treatment of OCD, are mainly medications that increase the amount of the neurochemical serotonin in the brain. The other option that is out there is therapy to try and lighten “the Load” as far as the rituals go. Even many Famous people have to cope with OCD such as Leonardo DiCaprio, Billy Bob Thornton, and Donald Trump. With the right management people can obtain a more fulfilling life then they had before. If a friend, family member, or even yourself is suffering from this disorder then get help as soon as possible or the effects will only get worse.
Social Anxiety Disorder (SAD) (or Social phobia)
David Bunch
Most people occasionally feel nervous meeting a new person or speaking in front of a group. People with social anxiety disorder (SAD), however, become overwhelmingly anxious and self-conscious even in everyday social situations. Theirs is an intense and persistent fear of being scrutinized by others or of doing something embarrassing. Even though they may find their own anxiety unreasonable, they can't overcome it by themselves.
What Causes Social Anxiety Disorder?
Social anxiety disorder typically begins during the teenage years and continues into adulthood. People may develop the disorder after a childhood history of social inhibition or shyness. Others experience an abrupt onset after a very stressful or humiliating experience. Like many anxiety disorders, your genes may play a role. There is no single known cause of social anxiety disorder, but research suggests that biological, psychological, and environmental factors may play a role in its development.
Biological: Social anxiety disorder may be related to an imbalance of the neurotransmitter serotonin. If the neurotransmitters are out of balance, messages cannot get through the brain properly. This can alter the way the brain reacts to stressful situations, leading to anxiety. In addition, social anxiety disorder appears to run in families. This means that the disorder may be passed on in families through genes.
Psychological: The development of social anxiety disorder may stem from an embarrassing or humiliating experience at a social event in the past.
Environmental: People with social anxiety disorder may develop their fear from observing the behavior of others or seeing what happened to someone else as the result of their behavior. Also children who are sheltered or overprotected by their parents may not learn good social skills as part of their normal development.
Treatments and drugs
Social anxiety disorders typically persist for life, often coming and going. Treatment can help control symptoms and make the person confident and relaxed in social situations. The two most effective types of treatment are medications and a form of psychotherapy called cognitive behavioral therapy. These two approaches are often used in combination.
Psychotherapy - Cognitive behavioral therapy improves symptoms in up to 75 percent of people with social anxiety disorder. This type of therapy is based on the idea that a persons own thoughts, not other people or situations, determine how they behave or react. In therapy, people learn how to recognize and change negative thoughts about themselves. Cognitive behavioral therapy may also include exposure therapy. In this type of therapy, you gradually work up to facing the situations you fear most.
Medications - Several types of medications are used to treat social anxiety disorder. However, selective serotonin reuptake inhibitors (SSRIs) are generally considered the safest and most effective treatment for persistent symptoms of social anxiety. SSRIs your doctor may prescribe include:
- Paroxetine (Paxil)
- Sertraline (Zoloft)
- Fluvoxamine (Luvox)
- Fluoxetine (Prozac)
Other medication options Your doctor or mental health provider may also prescribe other medications for symptoms of social anxiety, including:
- Other antidepressants. You may have to try several different antidepressants to find which one is the most effective and has the fewest unpleasant side effects.
- Anti-anxiety medications. A type of anti-anxiety medication called benzodiazepines (ben-zo-di-AZ-uh-penes) may reduce your level of anxiety. Although they often work quickly, they can be habit-forming. Because of that, they're often prescribed for only short-term use. They may also be sedating.
- Beta blockers. These medications work by blocking the stimulating effect of epinephrine (adrenaline). They may reduce heart rate, blood pressure, pounding of the heart, and shaking voice and limbs. Because of that, they may work best when used infrequently to control symptoms for a particular situation, such as giving a speech. They're not recommended for general treatment of social anxiety disorder.
first I am going to talk to you about what a phobia is. A fear or irritation that occurs in a certain situation, activity, thing, or person. Phobias can occur just by watching their reaction. The observer can take this experience and make it into a fear of just about anything.
The phobia I am highlighting is Glossophobia. Glossophobia is fear of speaking in front of the public. This fear is a very normal response to the stress of performing in front of a group of people. This fear could effect your life in the extreme. It can limit your career or even your relationships if you avoid it.
“ When giving a presentation to an executive, my panic was so severe I could not focus on his face and whole room seemed to be filled with fog. It was common for me to have an upset stomach before speaking to small groups. I had nightmares about discovering I was naked in front of people. When changing careers to one that required more public speaking, I spend days in bad in a fetal position, crying myself to sleep.”
This person has to deal with Glossophobia. There are thousands of other people who have to deal with this problem every single day, and it also effects their life every single day. There is nothing much more powerful than what we think others are going to think about us. Many of us choose what we wear, what kind of car you get, and what your house looks like by what other people think. We also choose our careers, friends, even our spouses based on what others think.
One of the main questions that runs through people’s heads that have Glossophobia would be, “What will people think if I say something stupid or stumble over a word or my clothes are messed up.” I’m sure there are plenty of other questions that go on in somebody’s head but that was just one. The more and more people think about their presentation or whatever public speaking they are going to be doing the worse the phobia gets. So whatever you do, don’t over think about your presentation. It will just make things worse.
Public speaking fear can be called many terms, like stage fright, speech anxiety, speech phobia, fear of speaking, or performance anxiety. It is a phobia that is socially related to self-presentation in front of an audience. Social anxiety is what most scientists call this phobia. There medical term is called glossophobia, which comes from the Greek words glossa and phobos. Phobos stands for fear or dread and glossa means tongue.
More men seek treatment to cure fear of public speaking than women. Some public speakers have turned to hypnosis therapy or beta-blockers to find relief. If you don’t take treatment then you could have some physical symptoms such as increased pulse, blushing, breaking out into a sweat, nausea, and eye contact difficulty.
What is Obsessive-Compulsive Disorder?
Chelsea Bryant
Obsessive-Compulsive Disorder is an illness that causes people to have unwanted thoughts, which are also called obsessions, and to repeat certain behaviors, or compulsions, over and over again. OCD has patterns of behavior get in the way of people’s daily lives. People with OCD know that their obsessions and compulsions make no sense, but they can’t ignore or stop them.
Obsessions:
Obsessions are ideas, images and impulses that run through a person’s mind over and over again. These thoughts are disturbing and cannot be controlled. Not all obsessions are constant, some people only have mild OCD, and their obsessions only happen once in a while.
Common Obsessions:
There are just a few of the common obsessions that people have:
Fear of dirt or germs
Disgust with bodily waste or fluids
Concern with order, symmetry, balance and exactness
Worry that a task has been done poorly, even when they know it has been done right
Fear of thinking evil or sinful thoughts
Thinking about certain sounds, images, words or numbers constantly
Need for constant reassurance
Fear of harming a family member or friend
Compulsions:
Compulsions are when people perform certain behaviors according to “rules” that they make up for themselves. People perform these behaviors because it is the only way that they can get the nervous feeling to go away for a short time, but then when the nervous feeling comes back they have to repeat the behavior all over again.
Common Compulsions:
These are just a few of the common compulsions that people have:
Cleaning and grooming, such as washing hands, showering or brushing teeth over and over again
Checking drawers, door locks and appliances to be sure they are shut, locked or turned off
Repeating actions, such as going in and out of a door, sitting down and getting up from a chair, or touching certain objects several times
Ordering and arranging items in certain ways
Counting to a certain number, over and over
Saving newspapers, mail or containers when they are no longer needed
Seeking constant reassurance and approved
In recent studies have proven that as many as 3 million Americans ages 18 to 54 may have OCD. This is only 2.3% of this age group though. OCD affects about 1 and 50 men and women. OCD can appear in childhood, adolescence, or adulthood. Normally OCD first shows up in the teens or early adulthood. Tests have proven that OCD more than likely runs in families. OCD symptoms may come and go, they may ease over time, or they can grow progressively worse the older a person gets. No one knows what the cause is for OCD. Research shows that OCD may be caused by chemicals in the brain that carry messages from one nerve cell to another. One of these chemicals is serotonin, which helps to keep people from repeating the same behaviors over and over again. When a person has OCD there body does not produce enough serotonin. There are some medicines that will increase the amount of serotonin in a person’s brain.
OCD can be treated with a combination of therapy and medication. There are several different medications available to help treat OCD. These medications are also often used for depression and include: clomipramine, fluoxetine, sertraline, paroxeine and fluvoxamine. These drugs can cause side effect, and it may take several weeks before your behavior improves. When people are in therapy their therapist encourage them to do things that make them nervous but tell them not to do their rituals that they usually do when they get nervous. It will take awhile for the nervous feeling to go away but the more they don’t do the rituals the better their nervousness will get. People with OCD must be able to tolerate the high levels of anxiety.
Post Traumatic Stress Disorder is a psychological disorder that affects some people who have faced difficult situations. It is an anxiety disorder that can become prevalent if you have faced life threatening or frightening situations.
PTSD can appear immediately following a traumatic event or it may be delayed for up to 6 months. If the symptoms of PTSD appear immediately they are easily treatable and will usually get better in a few months. However, if PTSD appears later the symptoms are much more intense and are more difficult to treat. PTSD can happen at any age following any traumatic event, such as, a natural disaster, a life threatening accident, war, abuse, rape, or losing family or friends. Events such as these will produce stress in everyone, but not everyone develops PTSD from these events.
It is unknown exactly what causes PTSD, but we do know that psychological, social, physical, and genetic factors are involved. PTSD affects a bodies' reaction to stress effecting the neurotransmitters carrying information to the brain along with messing up stress hormones, causing real panic and stress to trigger at just a memory of what was a stressful situation. PTSD is more likely to occur if one has been subjected to stress in the past.
Having PTSD causes the person suffering to re-live the traumatic event over and over again. In some PTSD sufferers this means vivid memories of the event or as stated before actually believing they are there again re-living the event, this is called a flashback. The memories or flashbacks can be triggered by simple everyday objects that may remind one of the event. People are less likely to develop PTSD when they have strong social support from family, friends, and others.
Symptoms
PTSD symptoms can be categorized in three main ways:
1. Reliving the event which disrupts daily life
• Flashbacks where the person finds himself re-experiencing the event again and again
• Recurring memories and dreams of the event
• Physical reactions to objects that remind the person of the event
2. Avoidance
• Emotional numbing, they feel as though they just don't care anymore
• Feelings of detachment from themselves
• Unable to remember important aspects of the traumatic event
• Lack of interest
• Less expression of their moods
• Staying away from people, places, or things that remind them of the event
• Believing they have no future
3. Arousal
• Difficulty concentrating
• Extreme reaction to fear
• Excessive awareness bordering on paranoia
• Irritability or outbursts of anger
• Difficulty sleeping
It is also likely that the person affected my have feelings of guilt known as “survivor guilt,” with symptoms like those that would come from anxiety, stress, and tension.
Treatments
Treatment for Post Traumatic Stress Disorder involves patients suffering from PTSD to recall the stressful event, express their feelings, and possibly learn to gain control over the event. In some cases expressing their feelings and mourning completes the mourning process and patients can carry out their lives. PTSD patients will often have support groups where they can talk out their stressful events with others who have similar problems. PTSD patients usually turn to drugs and alcohol to solve their problems so substance related issues must be treated first before PTSD can be treated.
DISSOCIATIVE IDENTITY DISORDER
By Patricia Rickard
Dissociative Identity Disorder (DID) or multiple personality disorder is a mental illness that is characterized by having two or more clear identities or alters. With DID a person is unable to connect to their own thoughts, memories and actions. The alters have their own age, race, or gender. Each one has different gestures, posture and tone of voice. These alters even have different ways of reacting, such as emotions, blood pressure and blood flow to the brain.
People with Dissociative Identity Disorder usually have other mental illness, such as Schizophrenia, psychosis and Delusions. Some even experience depersonalization (sense of being detached from self), derealization (world not real), amnesia (failure to recall personal information) and identity confusion or identity alteration (confused about who self is).
Although there is no proven cause to DID, some psychologists have a theory that the disorder is a reaction to severe trauma experienced as a child. The child is so severely traumatized that they dissociate themselves from the situation or bad experience. The DID becomes their coping mechanism or get way.
There are many Signs and Symptoms that a person with Dissociative Identity Disorder will experience.
-memory lapses (special occasions, life changing experiences)
-time loss
-encountering unfamiliar people who know them
-hallucinations
-flash backs
-depression
-being called different names
-hearing voices in their head
-not recognizing themselves
-feeling unreal
-feeling like more than one person
-mood swings
-suicidal thoughts
-sleep disorders
-substance abuse
-out of body experiences
With all these signs and symptoms it is difficult to diagnose because there is no definitive test. Practitioners conduct a mental-health interview to gather information. They gather facts about the person’s childhood and look at signs and symptoms. If the symptoms cannot be linked to any other mental disorder then the person is diagnosed with DID. This process takes time, most are in the mental health system for seven years before ever being diagnosed.
Although there is no cure for DID, there is help to cope with the disorder. The main component of treatment is Psychotherapy. This involves helping clients to improve relationships, preventing crises and experiencing feelings they are not comfortable with.
Hypnosis is another treatment sometimes used to help DID patients learn more about their alters. Learning more about their alters may give them better control over their different personalities.
Medications can be helpful too. The effects however may make the patient feel as if they are being controlled. This can cause further trauma.
People who do not seek help are vulnerable. They are at risk for attempting suicide more than once, abusing illegal substances and alcohol to cope and having violent behaviors. Most are incapable of maintaining a job or relationship. Overall they have a lower quality of life.
It is unsure how many actually live with Dissociative Identity Disorder. The overlap of symptoms it has with other disorders sometimes results in misdiagnosis. This has led to a disagreement among professionals. Some are unsure if the disorder even exists.
Borderline personality disorder is when people have a long pattern of unstable or turbulent emotions like feelings about others and themselves. They can take impulsive actions and many times they won’t have a stable relationship. The causes of Borderline Personality disorder, or BPD, are still unclear and unknown. They do know that Genetics, family, and social factors can play a role. There are many risk factors that come with BDP. Research shows that some major factors that play a role with people being diagnosed with BPD reported a history of abuse, neglect, or separation from parents in their childhood. 40-70% of people with BPD reported being sexually abused.
BDP occurs more often in women and also among hospitalized psychiatric patients.
The symptoms of BDP include:
1) They are uncertain about themselves and because of this their intrests and values change rapidly
2) Things that we consider bad, they consider extremely bad and their views of a person changes rapidly.
3) Fear of being abandoned
4) Feelings of emptiness and boredom
5) Frequent displays of inappropriate anger
6) Impulsiveness with money, substance abuse, sexual relationships, binge eating, or shoplifting
7) Intolerance of being alone
8) Repeated crises and acts of self-injury, such as wrist cutting or overdosing
BDP is diagnosed based on a psychological evaluation and the history of their symptoms.
Treatment
1) Dialectical Behavioral Therapy, or DBT, can successfully treat this disorder. Group therapy can also help them control and change their self-destructive behaviors.
2) Medication can help with the mood swings and also help treat their depression
Complications:
1) Depression
2) Drug abuse
3) Problems with work, family, and social relationships
4) Suicide attempts and actual suicide
We all know that person. You know the one, living in the gray area between free and being in prison, not holding a job for over a few months at a time, always having alcohol or drugs or toys no matter if the family has no shoes or nice clothes, everything that “happens” to them is someone else’s fault and the world is always out to get them. You know, not the person who has a bad week or two, but has been this way since high school. People living like this suffer from a disorder called “antisocial personality disorder”.
What is Antisocial Personality Disorder? The following is from DSM-IV-TR, a book used by mental health providers for disorder diagnosis.
(DSM-IV-TR Diagnostic Criteria for Antisocial Personality Disorder (301.7))
There is a pervasive pattern of disregard for and violation of the rights of others occurring since age 15 years, as indicated by three (or more) of the following:
1. failure to conform to social norms with respect to lawful behaviors as indicated by repeatedly performing acts that are grounds for arrest
2. deceitfulness, as indicated by repeated lying, use of aliases, or conning others for personal profit or pleasure
3. impulsivity or failure to plan ahead
4. irritability and aggressiveness, as indicated by repeated physical fights or assaults
5. reckless disregard for safety of self or others
6. consistent irresponsibility, as indicated by repeated failure to sustain consistent work behavior or honor financial obligations
7. lack of remorse, as indicated by being indifferent to or rationalizing having hurt, mistreated, or stolen from another
B. The individual is at least age 18 years.
C. There is evidence of conduct disorder with onset before age 15 years.
D. The occurrence of antisocial behavior is not exclusively during the course of schizophrenia or a manic episode.
Let’s look closer at the seven criteria listed above.
1. failure to conform to social norms with respect to lawful behaviors as indicated by repeatedly performing acts that are grounds for arrest . These people do what ever they want whenever they want. Offences as petty as traffic violations; speeding, wreckless driving, driving under the influence and driving without a licence are common place. Many do not have a driver’s licence due to repeated traffic offences and still drive anyway. Driving under the influence many times indicates an abuse issue, which we will discuss later.
2. deceitfulness, as indicated by repeated lying, use of aliases, or conning others for personal profit or pleasure. These people, as we will see on item 6, hold jobs for short periods of time, therefore money is an issue, These people always have a need, be it real or not, and when they do convince family, friends or lending institutions to ‘loan’ them money; the money rarely gets used for the intended purpose, is never repaid and there is no gratitude for the money.
3. impulsivity or failure to plan ahead. These folks, refer back to #1, do what they want when they want with out any regard to consequences. They don’t worry about the money that was supposed to pay the rent or groceries. They don’t think of the fact they don’t have a drivers licence, etc.
4. irritability and aggressiveness, as indicated by repeated physical fights or assaults. Looking at numbers 1 and 3 it is not surprising to see the irritability show up. People around the ASD person get very tired of being used and abused and sooner or later begin telling this person what they think and start cutting off the support that has been provided. This is the point, many times, the ASD person starts getting physically violent and more run ins with law enforcement become more serious.
5. reckless disregard for safety of self or others. Many persons with ASD partake in increasingly more dangerous activities. For instance the aggression and fighting or running from law enforcement. The need for more stimulation is somewhat like an addict’s growing tollerence of the drug of choice and needing more to achieve the same result.
6. consistent irresponsibility, as indicated by repeated failure to sustain consistent work behavior or honor financial obligations. Many of these people move from job to job as they simply do not accept the responsibility of the job. Many times the family structure is destroyed as one parent with ASD is not trustworthy enough to care for the children while the other parent tries to work to keep a roof over their head and food on the table. A big problem as the lack of discipline is one of the suspected causes of ASD, therefore creating another generation with the disorder.
7. lack of remorse, as indicated by being indifferent to or rationalizing having hurt, mistreated, or stolen from another. And last but certainly not least, total lack of regard for the feeling of others. Stealing the grocery money for beer or drugs and not feeling any remorse when the children are hungry and there is no food.
Antisocial personality disorder has no blood test or chemical markers to show ASD. Diagnosis is made by a mental health practitioner conducting an interview and assessment on the individual, the above s/s being observed the practitioner still must take into account the individual’s culture. The diagnosis of ASD will not usually be made on people under the age of 18 years of age, however the s/s of ASD must have been present and observable since the person was at least 15 years of age.
So, what causes antisocial personality disorder? Dr. Donald Black writes on www.psychcentral.com that the cause(s) of ASD is/are thought to have origins in ones heredity and environment. The doctor also feels the environmental factors play as much a role as does the heredity.
Some of the abnormal nervous system development signs include learning disorders, persistent bedwetting and hyperactivity. Adrian Raine, DPhil, from the University of Southern California and colleagues compared MRI’s of ASD patients with those who do not exhibit ASD symptoms and signs and found an 11% reduction of frontal lobe mass of the brain in the ASD group. This may explain the low arousal level, poor fear conditioning, lack of conscience and decision making deficits that many ASD people exhibit.
Some environmental issues cited by Dr. Black are mothers who smoked during pregnancy, parents who exhibit antisocial behavior, families suffering from a parent(s) with alcoholism, substance abuse, criminal activity and dysfunctional family marked by frequent separation, absence of a parent and divorce.
Family discipline and supervision are linked as well to antisocial behavior in children. Parents who are involved in their children’s lives tend to monitor behavior, set rules and see the rules are obeyed, make sure they know the child’s whereabouts and steer the children away from situations such as troubled playmates and situations the child would be negatively influenced. Many times in broken homes parents may not be available to supervise the children or have a network in place to assure proper supervision. Antisocial parent(s) often lack the motivation to supervise their children thereby giving the child a positive reinforcement that antisocial behavior is not only tolerated but acceptable.
Early abuse to the child has also been considered harmful. An action such as vigorously shaking a child may result in injuring the brain and disrupt normal development of the central nervous system. This disruption may continue through the adolescent years. The injury could cause the release of hormones and other brain chemicals during stressful events altering the pattern of normal development. Other traumatic abuse during childhood include physical abuse, mental abuse as well as sexual abuse.
What can be done to ‘cure’ this disorder? Sadly ASD does not have a ‘magic pill’. People with this disorder can learn healthy ways to deal with the anxiety and impulses, unfortunately this takes a significant commitment of time and therapy. Nearly all people suffering ASD only attend therapy under duress from a court order and as soon as the court order is fulfilled the counseling stops and life continues as before. Some attend counseling under coercion from spouse or marriage counselor and this just adds to the problem of anxiety and impulsive actions.
Here in America drinking is socially acceptable and alcohol is readily available but it is also the most commonly abused drug in America. Alcoholism is a chronic disease characterized by the person’s inability to control his or her craving for a drink and their dependence on alcohol to feel “normal”. According to drug-addiction-support.org, Alcoholism is very progressive. It begins with one drink to be sociable, or to try to enjoy the effects of alcohol, but progresses to the point where the person needs more alcohol to achieve the same effect.
According to medicine.net the effects of alcoholism can be very serious. Here are some of the consequences of excessive drinking, cancer of the liver, esophagus, throat, and larynx. Other effects are liver cirrhosis, immune system problems, brain damage and harm to the fetus during pregnancy. There is also an increased risk of death from automobile accidents, recreational accidents, and on-the-job injuries. Additionally both homicides and suicides are more likely to committed by a person who have been drinking. Furthermore, alcohol-related problems cost society approximately $185 billion per year.
What is Alcoholism? Alcoholism is also known as “alcohol dependence” which is a disease that includes four symptoms. Craving: a strong need, or compulsion, to drink, loss of control the inability to limit one’s drinking on any given occasion, physical dependence withdrawal symptoms, such as nausea, sweating, shaking, and anxiety occur when alcohol use is stopped after a long period of drinking and tolerance the need to drink greater amounts of alcohol in order to get drunk.
Along with effects of alcoholism there are also severe symptoms such as: alcohol-related illnesses, a need for large amounts of alcohol to get drunk, blackouts, withdrawal symptoms, continuing to drink even when health, work, or family is being harmed, drinking, alone, violent episodes, lack of control, making excuses to drink missing work or school, no longer taking part in social activities, need for daily or regular alcohol use to function, neglecting to eat, not caring for physical appearance.
The hardest part of alcoholism is getting help and treatment. The decision to get help or getting treatment is very difficult. The person can easily be in denial and will not admit to having a problem with alcohol. There are numerous ways to get treatment. Some problem drinkers maybe successful with simply reducing the amount they drink. If drinking in moderation doesn’t work then person should try to be completely sober. Completely stopping alcohol intake and then remaining sober is difficult for many alcoholics. Alcoholism is treated as a chronic disease and patients should expect and accept relapse but should aim for as long a period without drinking as possible.
In conclusion alcoholism is a major issue facing American it is the most common drug addition. Controlling the amount of alcohol a person consumes can prevent it. Many people do over consume alcohol and that can be a major factor, which leads to alcoholism. So the next time you drink don’t drink to get drunk.
Have you ever tried talking to someone who rapidly changes emotions? For example, did said person rapidly cycle between being angry, happy, and sad all within a matter of seconds? If so, you have probably had conversations with someone who suffers from bipolar disorder, also known as manic-depressive disorder. Being bipolar is a psychiatric condition that affects nearly 4% of the world’s population.
Bipolar disorder is a condition in which a person may experience unusually elevated states of emotion (hypomanic or manic phases), and depressed states of mind for periods of time that tend to disrupt everyday life for the person suffering from it. However, like most mental diseases, symptoms are not the same from patient to patient, and there isn’t an easy test to confirm or disprove that a patient has the disorder.
The depressive episodes are typically to be the first thing noticed in someone that suffers from bipolar disorder. Symptoms of the depressive phase that are typical in most patients include anger, despondency, guilt conscience, feeling alone, and general sadness. These symptoms are usually so severe that they disrupt all activities that were once found enjoyable, e.g. (Food, Sleep, and Sex.) In extreme cases, said individual can become what is known as psychotic. These psychotic phases typically focus around delusions, and they can last from anywhere between two weeks to even six months if the appropriate action isn’t taken.
Mania, a.k.a. manic episodes, is the hallmark of bipolar disorder. Also, the varying severity of the mania a patient suffers from is usually how the disorder is classified. Mania is not quite the opposite of a depressive episode, but it can include extreme bouts of euphoria. While it can include happiness, mania is generally characterized as a state of elevated energy. This unnatural energy extremely disturbs sleep patterns. It can even cause the patient to go for days without sleep. Judgment impairment is the worst part of a manic episode. This lack of judgment can cause the person suffering it to feel grandiose. This is shown through abnormal shopping sprees, increased sexual drive, and worst of all, the feeling of invincibility, e.g. (Thinking they were “chosen” by a god.) There is also a dangerous side to mania including, but not limited to, substance abuse, rage, or even a break with reality.
Bipolar disorder is not simply one disease. It is divided into three different subtypes: bipolar I disorder, bipolar II disorder, and Cyclothymia. Bipolar I is the most severe, and the most dangerous form of bipolar disorder. The mood swings caused by it can inhibit nearly every part of the patient’s regular life, disrupting work, relationships, and school. Bipolar II is not as severe as bipolar I since the manic mood swings never go into full-blown mania, but it is still a terrible burden to live with because the depressive periods last longer than the other emotional shifts. Cyclothymia is the easiest form to live with. It can still be disruptive to everyday life, but its highs and lows are not as severe as in the other two disorders.
Schizophrenia is a mental disorder characterized by disintegration of thought processes and of emotional responsiveness. It most commonly manifests as auditory hallucinations, paranoid or bizarre delusions, or disorganized speech and thinking, and it is accompanied by significant social or occupational dysfunction. The onset of symptoms typically occurs in young adulthood, with a global lifetime prevalence of about 0.3–0.7%. The data shows that based on observed behavior and the patient's reported experiences.
Genetics, early environment, neurobiology, and psychological and social processes appear to be important contributory factors. There are medications that can help control who are schizophrenia, but some of the prescription drugs appear to cause or worsen symptoms. Current research is focused on the role of neurobiology, although no single isolated organic cause has been found. The many possible combinations of symptoms have triggered debate about whether the diagnosis represents a single disorder or a number of discrete syndromes. Schizophrenia does not imply a "split mind" and it is not the same as dissociative identity disorder—also known as "multiple personality disorder" or "split personality"—a condition with which it is often confused in public perception.
The mainstay of treatment is antipsychotic medication, which primarily suppresses dopamine, and sometimes serotonin, receptor activity. Psychotherapy and vocational and social rehabilitation are also important in treatment. In more serious cases—where there is risk to self and others—involuntary hospitalization may be necessary, although hospital stays are now shorter and less frequent than they were.
The disorder is thought mainly to affect cognition, but it also usually contributes to chronic problems with behavior and emotion. People with schizophrenia are likely to have additional (comorbid) conditions, including major depression and anxiety disorders; the lifetime occurrence of substance abuse is almost 50%. Social problems, such as long-term unemployment, poverty and homelessness, are common. The average life expectancy of people with the disorder is 12 to 15 years less than those without; the result of increased physical health problems and a higher suicide rate are low like 5%.
Schizophrenia and MPD in Film
Recently, there has been a rise in the popularity of movies with characters that show signs of schizophrenia. The same can be stated about multiple personality disorder (MPD). The most recognizable film where schizophrenia can be seen is “Donnie Darko”. A couple examples of MPD in a movie would be “Fight Club” and “Me, Myself and Irene”, starring Jim Carrey and Renée Zellweger. There are many more Hollywood titles with examples of personality disorders such as “Sybil”, “A Beautiful Mind” and even “The Dark Knight”
“Fight Club” is a perfect example of an individual with multiple personality disorder, granted the narrators’ case is an extreme one. In the movie, the narrator, whose true identity is never revealed, is telling the viewer his story. It starts with him telling the viewer about how he deals with his everyday life, having insomnia. Eventually, soap salesman Tyler Durden appears and they become friends, Tyler telling the narrator his stories and various theories. The narrator and Tyler start a “Fight Club” where any man can join to escape the monotony and frustrations of everyday life. This “Fight Club” gathers more and more members and eventually fight clubs develop in several surrounding cities, which in turn become a networking system for Tyler Durdens’ “Project Mayhem”. As the story comes to an end, the viewer realizes that the narrator and Tyler Durden are on in the same person. Tyler is an alter ego created by the narrator to express his true feelings about the life he is living.
In the Batman movies, Bruce Wayne and Batman are two completely different people. Bruce Wayne is the CEO of Wayne Enterprises and leads a normal billionaire life. When he is not living the dream, Bruce becomes the anti-crime vigilante known as Batman. Wayne is very successful at hiding his true identity. When he becomes batman, there is no trace of Bruce Wayne; his character changes completely. He becomes mysterious, more courageous, and intolerant of wrong-doers when he puts on the suit and mask.
Donnie Darko is a troubled teen who has a history of violence and does not get along with many people, save a girl named Gretchen and his psychiatrist. In the “Donnie Darko” movie, Donnie escapes a bizarre accident involving a jet engine landing on his bedroom. He was not in his room due to following a man in an evil looking bunny suit outside. The rabbit, named frank, can only be seen by Donnie and is essentially an imaginary friend with an extremely distorted voice. The difference is; Frank tells Donnie that the world is going to end in 28 days and gets him into various odd and demented kinds of trouble throughout the remaining days. Donnie’s psychiatrist writes off Frank as an imaginary friend and later discovers that Donnie is in fact a schizophrenic. In the end, Donnie is seeing all of the events that have occurred as if travelling time. On the final day, Donnie is sleeping in his bed and gets killed when a jet engine crushes his bedroom.
Eating disorders are devastating behavioral maladies brought on by a complex interplay of factors, which may include emotional and personality disorder, family pressure, a possible genetic or biological susceptibility and a culture in which there is an overabundance of food and an obsession with thinness. One of these disorders is anorexia nervosa.
Anorexia is a mental problem manifested in a physical form. It is an eating disorder that causes people to intentionally starve themselves or severely restrict their food intake. Anorexia usually occurs at the time of puberty and involves extreme weight loss. People who have this disorder have a fear of becoming overweight even though they are 15% below the average weight. Many causes of anorexia show that they adhere to strict exercise routines to keep off weight, 90% of all anorexics are women.
Anorexia Nervosa means “nervous loss of appetite”. This meaning is not on the whole right, since it is based on misunderstanding. The people who bear from Anorexia Nervosa do not at all have lack of need to eat; they are only afraid of putting on weight. Therefore, the term “self starving” would be more appropriate, or even better expressed “weightfobia”.
The cause of anorexia is unknown, but people with this disorder believe that they will be happier and more excepted thin. These people tend to be perfectionist and have to have everything in their lives perfect. Many cases occur in good students that are involved in student activities and sports. Anorexics incorrectly believe that they need to lose weight to be happy. Body image distortions are common. Some cases of Anorexia occur from difficulties in relationships and unresolved conflicts or painful experiences from childhood.
Some of the symptoms:
• Deliberate self-starvation with weight loss
• intense fear of gaining weight
• refusal to eat
• denial of hunger
• constant exercising
• greater amounts of hair on the body or face
• sensitivity to cold
• absent or irregular periods
• loss of scalp hair
• a self-perception of being fat.
Health Consequences of Anorexia Nervosa: In anorexia nervosa’s cycle of self-starvation, the body is denied the essential nutrients it needs to function normally. Thus, the body is forced to slow down all of its processes to conserve energy, resulting in serious medical consequences:
• Abnormally slow heart rate and low blood pressure, which mean that the heart muscle is changing. The risk for heart failure rises as the heart rate and blood pressure levels sink lower and lower.
• Reduction of bone density (osteoporosis), which results in dry, brittle bones.
• Muscle loss and weakness.
• Severe dehydration, which can result in kidney failure.
• Fainting, fatigue, and overall weakness.
• Dry hair and skin; hair loss is common.
• Growth of a downy layer of hair called lanugo all over the body, including the face, in an effort to keep the body warm.
Inflicted damage and possible effects that anorexia may cause:
• Cardiac disease –The most common cause of death in individuals who are suffering from severe cases of anorexia.
• Bradycardia – A dangerous slowing of the heart rate that results from self-starvation.
• Brain Damage – Brain scans of anorexic patients have noted changes in brain structure as well as abnormal activity in parts of the brain. Some of this damage is reversible once an individual resumes a healthy diet, but certain impairments appear to be permanent.
• Dehydration – Can lead to kidney failure, heart failure, seizure, brain damage and death.
• Depression – Physical weakening can exacerbate the body dissatisfaction and self-loathing that are often at the core of anorexia cases. Suicide is believed to be responsible for as many as 50 percent of all anorexia-related deaths.
• Hyponatremia – The opposite of dehydration, drinking too much water can cause fluid in the lungs, brain swelling, nausea, vomiting, confusion, and death.
• Muscle Atrophy – A body that is deprived of essential nutrients will begin feeding on itself, depleting muscle mass (including heart tissue) in the process.
Treatment: Though anorexia nervosa can cause severe – even deadly – damage to a person’s physical, mental, and emotional well-being, the good news about this disease is that, with proper treatment, recovery is possible. If you suspect that someone you know is struggling with anorexia, do not hesitate to help them get the treatment that they so desperately need.
Anorexia Nervosa
Medical term for anorexia is Anorexia nervosa. It is when a human can’t stay at the minimum body weight for a healthy human at that age and height. Signs that you may have this disorder are if you are having extraordinary large amounts of fear about your weight and becoming fat when you are already underweight. If you haven’t had your period for three cycles or more. Most people with Anorexia nervosa refuse to admit seriousness of there weight loss. Because of the excessive weight loss there are many negative affects to Anorexia nervosa. These negative affects cause complications within the body. Some examples of this complication can be bloating, bone weakening, electrolyte imbalance, dangerous heart rhythms, decrease in white blood cells which leads to increased risk to infection, severe dehydration, severe malnutrition, seizures due to fluid loss from excessive diarrhea or vomiting, Thyroid gland problems which can lead to cold intolerance and constipation, hair falling out, and Tooth erosion and decay.
There is a similar disease called Bulimia nervosa. Bulimia nervosa and Anorexia nervosa are similar in that the subjects find themselves as being to “fat” even if they are underweight. People who suffer from Bulimia nervosa find themselves to still being over weight even if they eat just a small snack. Most start this mental disorder after they have been dieting and want to lose more weight then is needed. Bulimia nervosa is where instead of starving themselves they vomit the food, or take laxatives to get rid of the food from there bodies. They don’t lose there menstrual cycle as often as those who suffer from Anorexia nervosa. Because of the acid that is in the vomit, they tend to have higher rate of tooth decaying, and also have digestive mess ups from taking to many laxatives. Symptoms
Some symptoms of Anorexia nervosa are Blotchy yellow skin that is dry and covered with fine hair, brittle nails, depression, dry mouth, extreme sensitivity to cold, loss of bone strength, and wasting away of muscle and loss of body fat. Things others can watch out for are if someone is obsess about food, weight and dieting, they are overly strict about eating to few of calories then needed, exercise a lot even when they are sick or they are hurt, if they develop odd habits with food such as cutting it up into extremely small bite size pieces, or if someone become pulled away from there family and friends. They tend to fade from friends and family to hide there problem and keep it in secretly. They will also feel weak tired or faint often.
The term anorexia nervosa was established in 1873 by Sir William Gull which was one of the Queens personal physicians. It is a greek word, an- means denoting negation and orexis means appetite, put together they mean a lack of desire to eat. People who have Anorexia nervosa limit there amount of food to become dangerously thin. Less then 1% of the population are affected from this disease. Many people who suffer from anorexia are white and come from a wealthy family. However, it can happen to anyone.
Dani Dietz
The Cause of Anorexia Nervosa
Although anorexia nervosa mostly affects women, some men also suffer from this disorder and there are several reasons why. First, the push to be thin is seen everywhere. Television and magazines portray models and other celebrities as beautiful because they are so thin, therefore creating a trend that others want to follow. Second, traumatic events such as divorce, abuse, or death shatter people’s worlds and cause people to turn to anorexia. They feel like if they can’t control anything else in their world at least they can control their eating habits. The third reason people may become anorexic is because of a self esteem issue. Many people are teased about their weight during their school days and become anorexic to feel better about how they look. Last, many athletes are pushed into having perfectly lean, fit bodies causing them to turn to anorexia nervosa. It is important to remember that anorexia nervosa stems from deeper problems such as depression, loneliness, insecurity, pressure to be perfect, or feeling out of control. Treatments for Anorexia Nervosa
Many people suffering from anorexia nervosa remain quite and don’t let others know, not wanting to admit that they have a problem, so it is up to friends and family to help them. If you see signs of anorexia in a friend or family member you can call the National Eating Disorders Association at 1-800-931-2237 for referrals, information, and advice on what to do. It is important to not make accusations or throw scare tactics in a person with anorexia nervosa face because it will only cause them to further deny it, or cause more stress and emotions that trigger it in the first place. Treatment of anorexia comes in three steps beginning with changing how one feels about themselves and food by admitting they have a problem. The next step involves getting the person to eat more food, which will lead to the last step of getting to, and maintaining, a healthy weight. Unfortunately, for some suffering from anorexia nervosa, admitting they have a problem doesn’t come until they have been hospitalized because they are at a critically low weight and their body is wearing down because of malnutrition. Getting to the next step can be helped by getting a nutritionist or dietician that can teach healthy eating patterns as-well-as proper nutrition. A nutritionist can even make a meal plan so the person with anorexia can easily follow a planned calorie intake to get to a healthy weight. The hardest part is maintaining that healthy weight when you get there, which usually takes counseling to achieve. A counselor or therapist can help determine the inner problems or emotions which cause the diseased to turn to anorexia. It is hard for anorexic’s to change their view on themselves and many will still not think themselves skinny enough or will try to find flaws in their appearance. Many times when suffering individual’s look in the mirror they actually don’t see themselves as they are, but rather a person with fat or really any undesirable quality. It is important to be patient and most of all give support and be there for anyone you know who may have anorexia nervosa or any eating disorder for that matter.
Karen M. Unruh
The term biofeedback was coined in the late 1960s which described laboratory procedures that were conducted on subjects to train them to alter things such as heart rate. Biofeedback is another form of medicine which can help you control you bodily functions. You control functions such as heart rate by using your mind. You are hooked up to sensors that tell you information about your body. By using this information you can have the power to be able to reduce pain by relaxing certain muscles. Biofeedback is used to treat many physical and emotional problems such as anxiety, high blood pressure, irritable bowel syndrome and migraine headaches.
Scientists cannot explain how biofeedback works. Patients who can benefit from biofeedback are trained to relax and change their behavior. Relaxation is a very important part in treating people with conditions that are brought on by stress. Stressful situations produce strong physical symptoms such as increased heart rate, and high blood pressure.
A biofeedback machine allows patients to know what kind of activity is going on inside their body. One type of machine picks up electrical activity in the muscles and a flashing light bulb will go off. Patients then know and use their mind and thoughts to relax and reduce muscle tension and pain. A biofeedback therapist coaches patients and helps them relax. These techniques can be learned at home. A typical biofeedback sessions lasts 30 to 60 minutes. A patient may only need ten sessions but sometimes may need up to 50 sessions. This can become very expensive.
There are four different types of biofeedback. This first one is electromyography biofeedback. This type gives you information about you bodies muscle tension so you can practice relaxation. Thermal biofeedback is when sensors are attached to you fingers or feet to measure your skin temperature. Your temperature often drops when you are under stress; so a low reading can be a signal to start your relaxation techniques. Galvanic skin response training is when sensors are attached to you and measure the amount of perspiration on your skin, alerting you to anxiety. Heart rate variability biofeedback help you control your heart rate to improve blood pressure, lung function, and stress.
You can receive biofeedback therapy in physical therapy clinics and hospitals. Once being properly trained with biofeedback patients are now practicing biofeedback in the comfort of their own homes, by using portable devices which can connect to a computer. Before beginning biofeedback a patient should discuss it with their physician first. Doctors can help patients find biofeedback therapists in their area.
Biofeedback is appealing to patients. The procedure is noninvasive and patients have nothing to be afraid of and it has no adverse effects. It can reduce the need for medications and can be an answer for patients whose medications haven’t worked well, and most important it allows patients to take charge of their health and have some control over their bodies.
"Stare at the point on the ceiling and let your breathing become slow and deep.” This is the typical way that a session in hypnosis therapy starts. Research over the last forty years shows that hypnosis therapy is safe and effective, for many ailments; headaches, childbirth, improving concentration, quitting bad habits (i.e. cigarettes or chewing nails) are just a few of the things that it can help with. It can also serve as a mild anesthesia or help people to get over phobias. It can be used for many ailments which makes it a versatile treatment, unlike regular cognitive therapy or drug therapy.
Hypnosis as a therapeutic tool has probably been used throughout mankind. To completely understand hypnosis we must look back at ancient times. Hypnotism was largely used by village witchdoctors and shamans, through chanting and visualization rituals. Those healers believed that their rituals were based on the person being healed and how open they were to the treatment. Although hypnosis dates back to prehistoric times, the first visual documented use of hypnosis dates back to 3000 BC when the Egyptians used it in their sleep temples. Those temples became popular and continued to be in use through the Greek and Roman empires. The Bible also has accounts of hypnosis in it’s contents.
Anton Mesmer is known as the “Father of Hypnosis,” in modern society. He used his “magnetism” techniques to perform magical cures on people, but he was highly discredited by the people that investigated his techniques. In the early 1900’s a French pharmacist named Emile Coue developed his Laws of Suggestion, which was basically that the only people who would be hypnotized are the one’s who’s mind were open to suggestion. It wasn’t until 1958 that Milton Erikson brought hypnosis to the American Medical Association to be used for therapeutic needs.
Since Erikson, hypnosis has become a well known and practiced therapy in our society. It is not just a sideshow act at a circus, but a very good cognitive-behavioral therapy that is widely used today. The main pro of hypnosis therapy is that it does not hurt you at all; mind nor body. It is solely a healing device used to take care of habits and to make sure that your subconscious will not allow you to regress in whatever that you are trying to heal in your mind or body. How it works is simple. The first part of the therapy session consists of relaxing your mind and body. The therapist may send you to a “happy place,” and then begin the rest of therapy. The second half of your session with primarily be the therapist re-programming your subconscious so to speak. The way that they do this is through the power of suggestion, and while you won’t always remember what goes on in a session your subconscious will remember because that is what part of your mind is being spoken to. Hypnosis is a very good way to rid people of smoking and disorders that involve your subconscious. The uses for it today are very different than they used to be and that is mainly because of today’s technology.
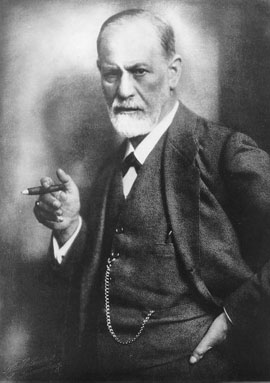

 Sigmund Freud, the father of psychoanalysis, was born on May 6, 1958 in Freiberg, Moravia. When he was four or five years old his family moved to Vienna, where he lived most of his life. Sigmund was a very smart child always at the head of his class. He attended medical school, where he began his research mainly focusing on neurophysiology.
Sigmund Freud, the father of psychoanalysis, was born on May 6, 1958 in Freiberg, Moravia. When he was four or five years old his family moved to Vienna, where he lived most of his life. Sigmund was a very smart child always at the head of his class. He attended medical school, where he began his research mainly focusing on neurophysiology.


















{kind=link}